Overview
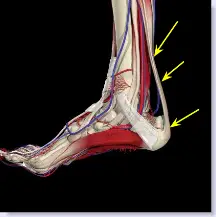 A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon.
A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon.
Causes
As with any muscle or tendon in the body, the Achilles tendon can be torn if there is a high force or stress on it. This can happen with activities which involve a forceful push off with the foot, for example, in football, running, basketball, diving, and tennis. The push off movement uses a strong contraction of the calf muscles which can stress the Achilles tendon too much. The Achilles tendon can also be damaged by injuries such as falls, if the foot is suddenly forced into an upward-pointing position, this movement stretches the tendon. Another possible injury is a deep cut at the back of the ankle, which might go into the tendon. Sometimes the Achilles tendon is weak, making it more prone to rupture. Factors that weaken the Achilles tendon are corticosteroid medication (such as prednisolone), mainly if it is used as long-term treatment rather than a short course. Corticosteroid injection near the Achilles tendon. Certain rare medical conditions, such as Cushings syndrome, where the body makes too much of its own corticosteroid hormones. Increasing age. Tendonitis (inflammation) of the Achilles tendon. Other medical conditions which can make the tendon more prone to rupture, for example, rheumatoid arthritis, gout and systemic lupus erythematosus (SLE) - lupus. Certain antibiotic medicines may slightly increase the risk of having an Achilles tendon rupture. These are the quinolone antibiotics such as ciprofloxacin and ofloxacin. The risk of having an Achilles tendon rupture with these antibiotics is actually very low, and mainly applies if you are also taking corticosteroid medication or are over the age of about 60.
Symptoms
The pain from an Achilles tendon rupture is usually felt in the back of the lower leg, in the area 2 to 6 cm. above the Achilles tendon's attachment to the calcaneus. Individuals with an Achilles tendon rupture often describe a "pop" or similar feeling at the time of the injury. A "hole" or defect in the Achilles tendon can usually be felt under the skin in this area. A limp and inability to rise up on the toes of the affected foot are usually present. If the affected foot does not plantar flex when the calf muscles are squeezed an Achilles tendon rupture is very likely.
Diagnosis
Some patients mistakenly believe the tendon is working if they can push the foot down, however, patients will usually be able to move the foot up and down while sitting because the other surrounding muscles and tendons are still intact. Trying to push up while standing and applying body weight to the foot will reveal the true weakness. Sensation and circulation to the foot and ankle will be normal. In addition, x-rays will be normal unless the Achilles injury involves pulling off (avulsion) of the bone on the calcaneus (heel bone). This is quite rare, occurring in only a small fraction of patients with Achilles injuries. Patients suffering this type of Achilles avulsion injury tend to be older with weaker bone. Imaging Studies. Plain x-rays will be negative in patients who have suffered an Achilles tendon rupture. The rupture can be seen on ultrasound or MRI. However, these studies are not indicated for acute ruptures unless there is some uncertainty about the diagnosis. For chronic problems of the Achilles or ruptures that are old, an MRI may be very helpful.
Non Surgical Treatment
Your doctor will advise you exactly when to start your home physical therapy program, what exercises to do, how much, and for how long to continue them. Alphabet Range of Motion exercises. Typically, the first exercise to be started (once out of a non-removable cast). While holding your knee and leg still (or cross your leg), you simply write the letters of the alphabet in an imaginary fashion while moving your foot and ankle (pretend that the tip of your toe is the tip of a pencil). Motion the capital letter A, then B, then C, all the way through Z. Do this exercise three times per day (or as your doctor advises). Freeze a paper cup with water, and then use the ice to massage the tendon area as deeply as tolerated. The massage helps to reduce the residual inflammation and helps to reduce the scarring and bulkiness of the tendon at the injury site. Do the ice massage for 15-20 minutes, three times per day (or as your doctor advises). Calf Strength exercises. This exercise is typically delayed and not used in the initial stages of rehabilitation, begin only when your doctor advises. This exercise is typically done while standing on just the foot of the injured side. Sometimes, the doctor will advise you to start with standing on both feet. Stand on a step with your forefoot on the step and your heel off the step. The heel and forefoot should be level (neither on your tip toes nor with your heel down). Lower your heel very slowly as low as it will go, then rise back up to the level starting position, again very slowly. This is not a fast exercise. Repeat the exercise as tolerated. The number of repetitions may be very limited at first. Progress the number of repetitions as tolerated. Do this exercise one to two times per day (or as your doctor advises).
Surgical Treatment
Operative treatment of Achilles tendon ruptures involves opening the skin and identifying the torn tendon. This is then sutured together to create a stable construct. This can be performed through a standard Achilles tendon repair technique or through a mini-incision technique (to read about the different types of techniques, look under Procedure in Achilles Tendon Repair). By suturing the torn tendon ends together, they maintain continuity and can be mobilized more quickly. However, it is critical to understand that the return to normal activities must wait until adequate healing of the tendon has occurred. The potential advantages of an open repair of the Achilles tendon include, faster recovery, this means that patients will lose less strength. Early Range of Motion. They are able to move the ankle earlier so it is easier to regain motion. Lower Re-rupture Rate. The re-rupture rate may be significantly lower in operatively treated patients (2-5%) compared to patients treated non-operatively (8-15%). The main disadvantage of an open repair of the Achilles tendon rupture is the potential for a wound-healing problem which could lead to a deep infection that is difficult to eradicate, or a painful scar.
A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon.Causes
As with any muscle or tendon in the body, the Achilles tendon can be torn if there is a high force or stress on it. This can happen with activities which involve a forceful push off with the foot, for example, in football, running, basketball, diving, and tennis. The push off movement uses a strong contraction of the calf muscles which can stress the Achilles tendon too much. The Achilles tendon can also be damaged by injuries such as falls, if the foot is suddenly forced into an upward-pointing position, this movement stretches the tendon. Another possible injury is a deep cut at the back of the ankle, which might go into the tendon. Sometimes the Achilles tendon is weak, making it more prone to rupture. Factors that weaken the Achilles tendon are corticosteroid medication (such as prednisolone), mainly if it is used as long-term treatment rather than a short course. Corticosteroid injection near the Achilles tendon. Certain rare medical conditions, such as Cushings syndrome, where the body makes too much of its own corticosteroid hormones. Increasing age. Tendonitis (inflammation) of the Achilles tendon. Other medical conditions which can make the tendon more prone to rupture, for example, rheumatoid arthritis, gout and systemic lupus erythematosus (SLE) - lupus. Certain antibiotic medicines may slightly increase the risk of having an Achilles tendon rupture. These are the quinolone antibiotics such as ciprofloxacin and ofloxacin. The risk of having an Achilles tendon rupture with these antibiotics is actually very low, and mainly applies if you are also taking corticosteroid medication or are over the age of about 60.
Symptoms
The pain from an Achilles tendon rupture is usually felt in the back of the lower leg, in the area 2 to 6 cm. above the Achilles tendon's attachment to the calcaneus. Individuals with an Achilles tendon rupture often describe a "pop" or similar feeling at the time of the injury. A "hole" or defect in the Achilles tendon can usually be felt under the skin in this area. A limp and inability to rise up on the toes of the affected foot are usually present. If the affected foot does not plantar flex when the calf muscles are squeezed an Achilles tendon rupture is very likely.
Diagnosis
Some patients mistakenly believe the tendon is working if they can push the foot down, however, patients will usually be able to move the foot up and down while sitting because the other surrounding muscles and tendons are still intact. Trying to push up while standing and applying body weight to the foot will reveal the true weakness. Sensation and circulation to the foot and ankle will be normal. In addition, x-rays will be normal unless the Achilles injury involves pulling off (avulsion) of the bone on the calcaneus (heel bone). This is quite rare, occurring in only a small fraction of patients with Achilles injuries. Patients suffering this type of Achilles avulsion injury tend to be older with weaker bone. Imaging Studies. Plain x-rays will be negative in patients who have suffered an Achilles tendon rupture. The rupture can be seen on ultrasound or MRI. However, these studies are not indicated for acute ruptures unless there is some uncertainty about the diagnosis. For chronic problems of the Achilles or ruptures that are old, an MRI may be very helpful.
Non Surgical Treatment
Your doctor will advise you exactly when to start your home physical therapy program, what exercises to do, how much, and for how long to continue them. Alphabet Range of Motion exercises. Typically, the first exercise to be started (once out of a non-removable cast). While holding your knee and leg still (or cross your leg), you simply write the letters of the alphabet in an imaginary fashion while moving your foot and ankle (pretend that the tip of your toe is the tip of a pencil). Motion the capital letter A, then B, then C, all the way through Z. Do this exercise three times per day (or as your doctor advises). Freeze a paper cup with water, and then use the ice to massage the tendon area as deeply as tolerated. The massage helps to reduce the residual inflammation and helps to reduce the scarring and bulkiness of the tendon at the injury site. Do the ice massage for 15-20 minutes, three times per day (or as your doctor advises). Calf Strength exercises. This exercise is typically delayed and not used in the initial stages of rehabilitation, begin only when your doctor advises. This exercise is typically done while standing on just the foot of the injured side. Sometimes, the doctor will advise you to start with standing on both feet. Stand on a step with your forefoot on the step and your heel off the step. The heel and forefoot should be level (neither on your tip toes nor with your heel down). Lower your heel very slowly as low as it will go, then rise back up to the level starting position, again very slowly. This is not a fast exercise. Repeat the exercise as tolerated. The number of repetitions may be very limited at first. Progress the number of repetitions as tolerated. Do this exercise one to two times per day (or as your doctor advises).
Surgical Treatment
Operative treatment of Achilles tendon ruptures involves opening the skin and identifying the torn tendon. This is then sutured together to create a stable construct. This can be performed through a standard Achilles tendon repair technique or through a mini-incision technique (to read about the different types of techniques, look under Procedure in Achilles Tendon Repair). By suturing the torn tendon ends together, they maintain continuity and can be mobilized more quickly. However, it is critical to understand that the return to normal activities must wait until adequate healing of the tendon has occurred. The potential advantages of an open repair of the Achilles tendon include, faster recovery, this means that patients will lose less strength. Early Range of Motion. They are able to move the ankle earlier so it is easier to regain motion. Lower Re-rupture Rate. The re-rupture rate may be significantly lower in operatively treated patients (2-5%) compared to patients treated non-operatively (8-15%). The main disadvantage of an open repair of the Achilles tendon rupture is the potential for a wound-healing problem which could lead to a deep infection that is difficult to eradicate, or a painful scar.
 RSS Feed
RSS Feed